
Octopi if the base word was Latin. It’s Greek, so octopodes for plural. Technically.
Because English is a bastard if a language octopuses and octopi are fine too.
Octopi if the base word was Latin. It’s Greek, so octopodes for plural. Technically.
Because English is a bastard if a language octopuses and octopi are fine too.
The leaves have begun to change in the south eastern US.

It may seem like that is the case for a bit, and often does to many patients. Myself included.
Keep in mind the target population is patients who are centralized sensitization patients. There are alpha channels of nerves that through real physical injury have created a feedback loop in the nervous system with the brain.
In these patients, who do have very real injuries, the pain levels are outside expectations for the things we can test, scan, see on imaging etc.
The mechanism is complex but essentially you can think of it as the nerve bundles of specific types are far more sensitive to stimuli and the brain becomes far more sensitive to signals received.
Breaking this feedback loop, which is often fed by avoidance of things, is important.
As for data, they have published papers in many journals with more than 20,000 patients who have been through the clinic showing progress improvement. Reductions in standard assessments for depression, improved mobility and exercise function, as well as removed reliance on medications / the polypharmacy causing underlying greater symptoms is proven in their large data set.
A lot of the mental model that has real impacts to physical symptoms revolves around breaking previously unrealized classic and operant conditioning that patients with this chronic pain sensitization often have present.
To correct and see the clear picture without clouding it, medications must be removed from the picture as polypharmacy issues can create a mess of problems that seem like they are bodily in origin but are in fact from the medication interactions.
It is a program vetted by the chronic pain treatment community for over 20 years, and the data is well reviewed, with every hour of the time a patient spends there carefully considered and measured for efficacy.
The program gets referral from many physicians in various other disciplines within and outside their hospital system for patients that meet their criteria.
To be clear, this is not a fly by night theory. It’s one of the best hospitals in the world with a program of pharmacists, doctors, PTs, nurses and supporting specialists who all meet daily per patient and make individual care plans. You seem them daily for hours a day. They monitor blood work and vitals as well as metabolic data as they taper medications. It’s deeply unpleasant but designed very intentionally to help. It does help.
Anecdotally, a patient story:
They came into the program malnourished, on a feeding tube, intense abdominal pain, GI bleeding, and on significant opiates to tackle pain levels from the GI issues.
On discharge, the patient had no expressed pain, was back to eating normally without the feeding tube, and was regaining weight . GI bleeding stopped.
6 months later they went back on pain medication from a pain physician and were right back in the ER with the same symptoms. Following the program’s instructions the same reversal took place again!
The power of the operant conditioning from taking medications when feeling symptoms is a powerful one that impacts the baseline arousal states of the parasympathetic and sympathetic nervous system. These impact all sorts of bodily processes which seem counter intuitive to apply to physical real problems, but the results speak volumes.
Everyone arrives a skeptic. I left seeing benefit in my life as a patient who these things apply to. I am not uneducated, I have created software to run clinical cancer trials for years. Yet even with that formal intellectual background I was missing things that had impact to my health condition. The average patient has less exposure to these things, and I spent 10 years seeking help for the pain before this from many physicians. Many things were tried. So all of that experience and exposure to alternative therapies and modalities to this one was brought in with skeptical critical analysis of their methods.
There is an element of trust required, and it is HARD, but the easy path of medicate or cut it out is often not the solution with patients like us. Since pain is very much a central nervous system process, treating as such makes sense.
Many chronic pain patients suffer from something called central sensitization.
I do, though didn’t really know about it in detail before finding a clinic that treats those patients.
I did 3 weeks at Mayo hospital’s pain rehabilitation clinic to run their program for patients that are all specifically central sensitization. You go in a bit blind not knowing what the program is, intentionally on their part.
It is run by several world class cognitive behavioral therapy doctors, and a team of nurses and physical therapists that work with you daily. It is… aggressive. You have no option to not do physical therapy or cardio, of which there is 2 hours and over 20 exercises to do every day. No matter how you hurt or feel. People who were there were all objectively seriously injured at one point and had like me real issues and real disabilities. The most empathetic thing that could do for you is to not acknowledge your symptoms and just make you do it.
They also took all and I mean ALL medications. Couldn’t have miralax. No advil. No gas medicine from the gas station. Nothing taken for symptoms. You could take things prescribed for conditions like aside reflux disease or insulin for diabetes, but nothing for how you felt.
So imagine having to do 2 hours of intense exercise, giving up all medications in about 3 days time, and doing things cold turkey for 3 weeks without any room to tap out. On top of that it is 35 hours a week of lectures on various topics related to the condition of centralized sensitization, chronic pain stress management, biofeedback, depression, anxiety, and skills to better enable you to live life.
They even held 1 hour sessions a week with family to summarize key lectures and give Q&A for them to help the patients be better supported in this weird chronic pain thing most families don’t understand.
It’s intense and not for everyone, but I went from being unable to do any physical activity, even walking the dog while I was taking pain medications and muscle relaxants etc. I went from that to biking 10 miles a day, at a 3:45 minute mile pace. I started their reconditioning program at 1 lb dumbbells doing curls for ten reps. I am now, 8 months after the program, curling 30 lb dumbbells and doing my own 2 hour workouts every week day.
I am still in incredible amounts of pain. They could not and will not fix the underlying causes physically or biologically.
However, they change patient lives with the CBT focus on how to live a more function filled life with chronic pain. They make us more active and better able to live a life worth living, within the constraints of moderate, sustainable, and adaptable.
Anyway, it changed me life and I would recommend it to anyone if they are in the long term battle with chronic pain. I saw specialists and got dozens of medications and scans for things. Surgical procedures, injections, blocks… you name it.
Only this worked to give me part of my life back.
Good luck to you
Had exact same fusion performed.
4 screws, 2 rods to connect them, and a 3-d sintered titanium cage between the vertebrae.
I can attest to the chronic pain and wanting to armor a bulldozer
smart enough to have a suppressor…
That is all of a form 4 stamp and a $200 check my man. These days it’s a few weeks dwell time.
I have 12 of them. Most of the guys I shoot with have several. None of them are even close to being on this side of the bell curve for intellect.
Dude had a plan that was well thought out, but the can on his pistol wasn’t an indicator of it.

What does that have to do with the comment I was responding to then?
Ok, but we already gave him the money 5 years ago.
So, what changes by selling it?
I bought one when no other option for an EV really existed for reasonable range batteries.
I have never owned a luxury car. My other car is a Honda accord from 2016.
I would be happy to have any other car brand, but the cost to replace the car with a different EV of similar range would cost us $30k. Is it really that important to harm yourself financially to signal to others your preferences for a person?

I was at the Mayo Hospital’s own chronic pain rehabilitation clinic, and have all the PT exercises they had their patients all do if interested.

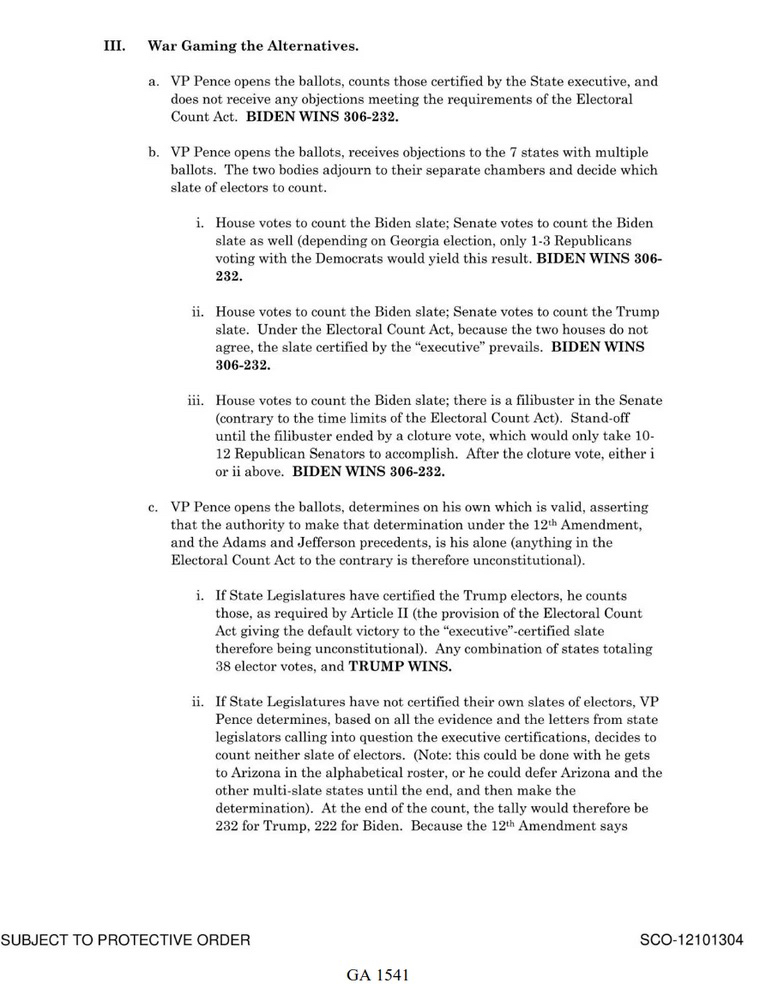
They wrote. It down.
It may prove to not end in consequences, but they took notes on a criminal conspiracy before the outcome and it’s part of evidence submitted in federal court.
Nothing burger is not nothing.

If your portfolio was a Fidelity target date fund, it would not be impacted by the local industry you mention in your post.
I also happen to know more about the details of how our retirement fund recommendations to clients works at Fidelity… because I worked there for the last 5 years.
You are showing the results of poor selection on your part.
As much as this is the dream, she is not electable in American politics for president.

Worked at a major company you would instantly know the name of.
They were a large corporation but were not public ally traded. Trillions of dollars in assets with more than 60k people employed.
DEI was a MAJOR push, with not just required corporate training but also sessions held often for minority groups of all types to speak their minds in forums about how to connect with them etc.
DEI initiatives and campaigns were a thing, VP of DEI was hired and they had a whole subsection under HR. Corporate events, entertainment, whole virtual bands playing to the theme of inclusion.
This same company did nothing when facing the burning obvious culture of being yes men to their bosses. They did nothing different than most any other massive rich company for how they treated workers, tracking their activity, location, and even physical assess login to buildings for reviews or as excuse to fire.
In an large address by a major leader in the organization I personally gave virtual written innocuous feedback, that they asked for, only to have that be met within minutes with being told never to do that again. The message wasn’t even seen by the speaker. It was just purely culturally unacceptable to offer any constructive criticism of any kind to people in high enough authority.
More than half a dozen people messaged me to tell me they appreciated I gave it public ally and it needed saying. I didn’t know any of them.
So if people are so important and we value voices being heard equally so much, why would you have people desperate to be treated like people and any such statement be met with greats of reprisal?
Yeah. DEI is fan fare in the same way the office cafeteria and gym were. They are designed to entice talent to come or stay while costing the company minimal amounts to do so.
What did I tell you about making up animals?
The numbers I gave are the model outputs for the state as of yesterday off his subscriber based model talk page.
So no.
Of course these are the likelihood of a win and not polling differences. That’s why I said model output, not a poll aggregate.
An 8 point spread in a state for polling averages is incredibly large. For reference Ohio is as deeply spread red in polling averages as Nee Jersey is blue. You think New Jersey votes red this year in any reasonable reality? No.
For an even more crazy but accurate comparison: Alaska has the same mid point statistical odds of going red as Ohio, but its error bars are more than double Ohio. Meaning? There is an incredibly slim but massively more possible chance Alaska goes blue than Ohio.
Current model from Silver and the polls raw data averages say it’s not even close. Trump will win the state by a 97.6% to 2.4% spread.
Because so many of you cannot understand modeling vs polling averages… that is the likelihood of a win as a result of taking poll inputs through Silver’s model, reflecting overall chances of a win as a output.
It is NOT polling average percentages.


I don’t want to type for ages here, but as someone who has been a sufferer and then medical patient for chronic daily migraines for decades; it actually is pretty nuanced.
For people like me, their chronic migraines are triggered as a secondary effect from the primary source. My headaches are called cervicogenic headaches, and migraine abortives like Obrelvy or Triptans are often used to arrest the storm. However, they are caused in origin from the occipital nerve, of which there are 3 branches in the neck.
An occipital nerve block is one commonly used tool, but it is often down blind without ultrasound. It is effective as hell at stopping migraine pain, and headache pain from what is the irritation or entrapment of occipital nerves. It has been common practice for several neuro and pain clinics I have seen for the last 2 decades. Problematically, they are not often offered in the emergency room setting because they are rather specialized procedures that usually are done by a neurology or trained pain physician. So that makes the emergency department a place that you go when the pain has overwhelmed all your other medications and resources, only to be met by not being able to get the one procedure that offers guaranteed relief for up to 2 weeks if given the block with steroids as well as local anesthetic. Frustrating to say the least, since you can plan on when you will get a massive headache, but you have to schedule to procedure weeks to months out with specialists.
Other migraine or occipital neuralgia triggering migraine treatments include other more invasive procedures to the nerves called ablations. Because cutting he nerve or surgically modifying them would result in scar tissue that would cause more problems or block regrowth, occipital ablations involve a needle slowly guided into the nerve under ultrasound imaging, and then they push electrical current into the needle while it is moved around by the provider. These can’t be numbed because you have to give feedback on where the currents are flowing in order to get it properly placed. Hurts like medieval torture. Then once placed they turn in ultrasonic pulses that heat the tip of the needle inside the nerve. This gets the tip hot enough to denature the nerve cells and kill them without harming the nerve sheath and allowing regrowth without nerve pain. It’s torture though and must be scheduled every 6-12 months. It doesn’t treat acute attacks, and can’t help with all types of headaches.
So offerings in the medical community pushed from specialized scheduled care to the responsive emergency providers as accepted medical interventions can be a massive improvement in accessibility to a treatment that can offer relief when no other physical interventions are reasonably possible for rapid abortive relief.